Naltrexone and Acamprosate are widely used to treat alcohol use disorder (AUD)–
- Naltrexone: Associated with a greater cumulative number of days of abstinence, fewer drinks, and less severe craving. Studies have shown it can be safe in patients with cirrhosis, including compensated and decompensated forms.
- Acamprosate: Associated with more frequent relapse compared to naltrexone, although it is effective when abstinence is required before treatment begins.
The importance of liver health–
- The choice of medication in patients with cirrhosis is complex due to the liver’s role in drug metabolism and the potential for liver damage.
- Studies have shown that naltrexone can be safe for patients with cirrhosis, even those with decompensated cirrhosis.
- Some research suggests naltrexone may even have a beneficial effect on the liver by reducing ALT/AST levels, liver fibrosis, and hepatitis.
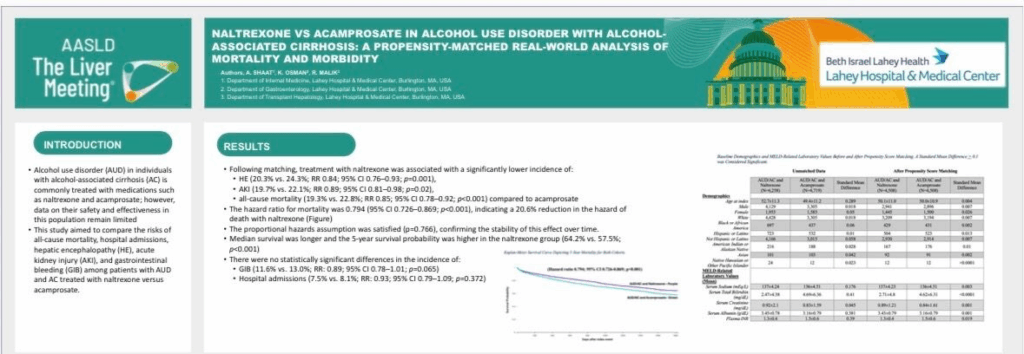
Recent studies (including the below poster from AASLD TLM 2025) could lead to a shift in prescribing patterns, with a greater emphasis on naltrexone in this patient group, which could potentially improve outcomes in terms of both morbidity and mortality. “
The study’s findings are significant because they provide evidence for the use of naltrexone in patients with alcohol-associated cirrhosis, a population that is often excluded from clinical trials.
✅ KEY POINTS
- MAUD (medications for alcohol use disorder) in patients with liver disease
- There is recognition that treating AUD in patients with advanced liver disease (including cirrhosis) is critically important for improving survival, but uptake of pharmacotherapy is low.
- A recent study (‘Safety of naltrexone in patients with cirrhosis’) in a U.S. Veterans cohort found that naltrexone initiation in patients with cirrhosis (n≈2,940 with labs) was not associated with drug-induced liver injury (DILI) based on RUCAM criteria.
- A UK real-world analysis of acamprosate use in patients with alcohol-related cirrhosis/alcohol-associated hepatitis found that in the matched cohort (53 acamprosate vs 53 controls) at 1 year: readmission was higher in the acamprosate group (85 % vs 57 %; p<0.001), and there were no statistically significant differences in abstinence or mortality.
- General AUD pharmacotherapy evidence
- For general AUD populations (not necessarily with cirrhosis), meta-analysis shows both naltrexone (50 mg/day oral) and acamprosate are associated with improved alcohol consumption outcomes compared with placebo (e.g., return to any drinking).
- However, the evidence on hard outcomes in liver disease (mortality, liver decompensation) is much weaker/not well established.
⚠️ KEY FINDINGS
- In the UK cirrhosis cohort, acamprosate did not confer a mortality benefit at 1 year, and was associated with higher hospital readmission.
- In the U.S. Veterans cirrhosis cohort, naltrexone appeared safe (i.e., no new DILI) but this study did not focus primarily on mortality/morbidity outcomes (decompensation, survival) in the AUD + cirrhosis context.
- There is no clear data to demonstrate one agent (naltrexone vs acamprosate) is superior in the AUD + alcohol-associated cirrhosis population for mortality or liver-morbidity outcomes (based on what’s publicly accessible).
🎯 The LiverRight Approach
There remains a need for rigorous real-world analyses (or ideally RCTs) of MAUD in the cirrhosis population with outcomes including survival, liver decompensation, transplant listing, etc.
Given the very high risk in alcohol-associated liver disease of decompensation, HCC, mortality etc., the utilization of AUD pharmacotherapy is a core component of our AUD care protocol.
While acamprosate has the advantage of minimal liver metabolism (so theoretically safer in advanced liver disease), the UK data suggests that in a cirrhosis cohort the benefit (abstinence/mortality) was not demonstrated and readmissions were higher (possibly due to confounding severity of AUD).
Naltrexone historically has been avoided in liver disease due to concerns about hepatotoxicity, but newer real-world evidence suggests it may be safe even in compensated and decompensated cirrhosis.
Because comparative data are lacking, agent selection in AUD + cirrhosis typically needs to be individualized (consideration of renal vs hepatic function, side-effect profiles, presence of opioid use, degree of liver decompensation, patient preference).