Consider “Association of food insecurity with MASLD prevalence and liver-related mortality” from the Journal of Hepatology, 2025.
The Net Net
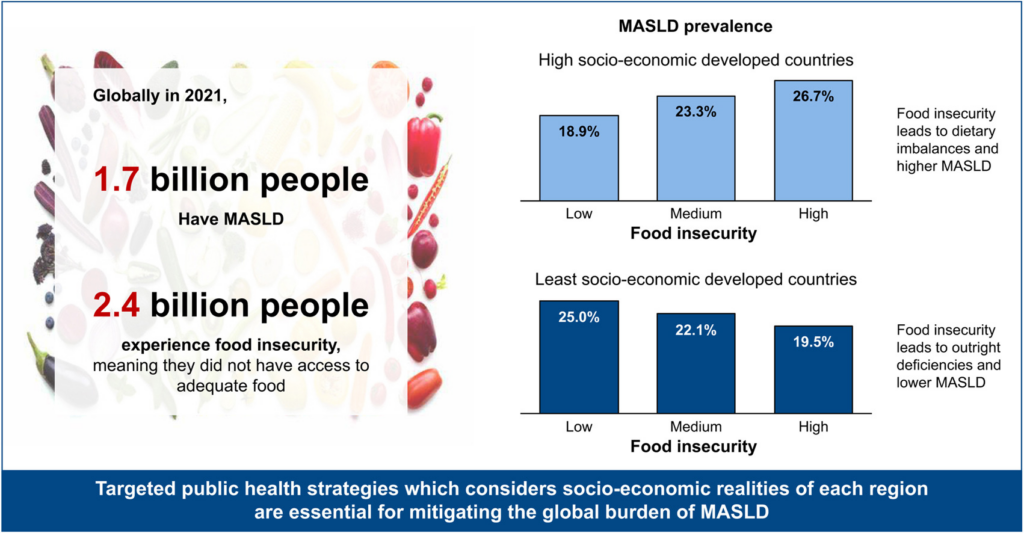
The study shows that food insecurity is strongly linked to the global prevalence of metabolic dysfunction–associated steatotic liver disease (MASLD), but the relationship differs depending on a country’s socioeconomic status.
Study Overview
Goal:
To examine how food insecurity relates to MASLD prevalence and liver-related mortality worldwide.
Data sources
- Global Burden of Disease (GBD) 2021 dataset
- United Nations food security indicators
- Analysis across 204 countries using statistical models that accounted for socioeconomic differences.
Major Findings
1. MASLD is common globally
- Median global MASLD prevalence ≈ 21.8%.
- Median MASLD liver-related mortality ≈ 2.9 per 100,000 people.
Regional differences were large:
- Highest prevalence: North Africa & Middle East (~41.7%).
- Lowest prevalence: high-income regions (~17%).
2. Metabolic risk factors remain the main drivers
Higher MASLD prevalence was strongly associated with:
- Obesity
- Type 2 diabetes
- Low physical activity
These metabolic risks were the strongest predictors of disease.
3. Food insecurity influences MASLD — but differently by country income
The relationship changes depending on socio-demographic index (SDI):
High-income / high-SDI countries
- More food insecurity → higher MASLD prevalence
- Likely explained by cheap ultra-processed food consumption.
Low-income / low-SDI countries
- More food insecurity → lower MASLD prevalence
- Likely due to undernutrition rather than caloric excess.
This highlights two very different nutritional pathways leading to liver disease.
4. Liver-related mortality is less influenced by food insecurity
Mortality was more strongly associated with:
- Age
- Obesity
- Metabolic comorbidities
rather than food insecurity alone.
Conclusion
The global burden of MASLD is shaped by both metabolic risk factors and socioeconomic conditions, including food insecurity. Effective public-health strategies must be tailored to regional realities (e.g., improving diet quality in high-income settings and addressing undernutrition and healthcare access in low-income regions).
✅ Why this paper matters (clinically):
- Shows MASLD is not only a metabolic disease but also linked to social determinants of health.
- Suggests food policy, nutrition access, and health equity interventions could reduce liver disease burden.
Graphic from the article–