Here’s a concise summary of the article titled “FIB-4-based Referral Pathways Have Suboptimal Accuracy to identify Increased Liver Stiffness and Incident Advanced Liver Disease” from July of 2025, as published in Clinical Gastroenterology and Hepatology.
The researchers evaluated how accurate FIB‑4-based referral pathways are at identifying liver disease—specifically significant liver stiffness measured by light-scattering methods—in low-prevalence populations (i.e., the general population).
The Key Findings
The study revealed that using FIB‑4 criteria for referrals:
- Fails to detect a substantial portion of patients with elevated liver stiffness:
- ~60% of individuals with liver stiffness ≥ 8 kPa
- ~50% of those with stiffness ≥ 12 kPa
- ~40% with stiffness ≥ 15 kPa
- ~25% of those who later develop advanced liver disease
Real Implications
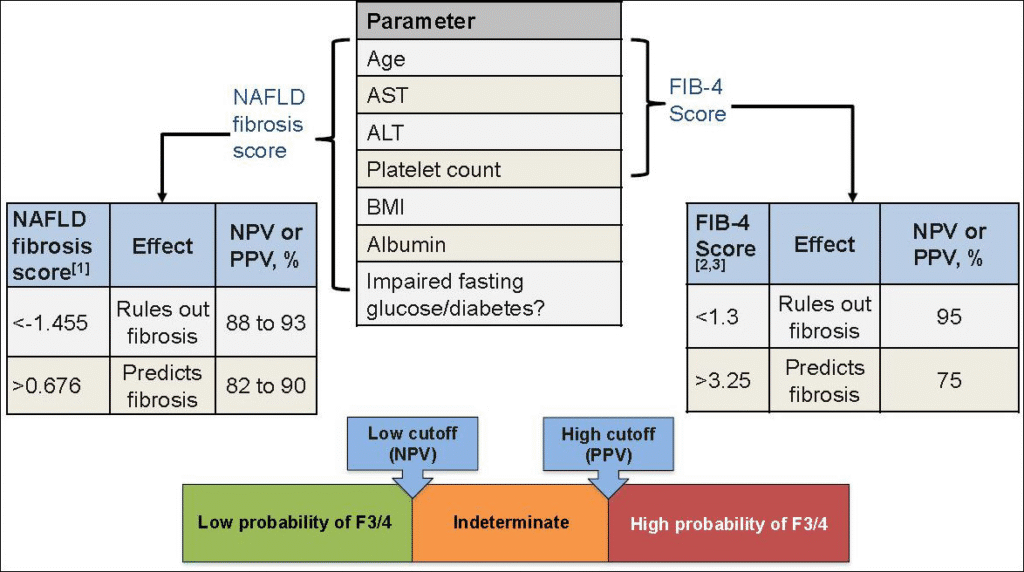
FIB‑4, a non-invasive and easily calculated tool based on laboratory values (age, ALT, AST, and platelet count), appears to underperform when used as a screening method in general populations that have a low baseline risk for liver disease.
Its limited sensitivity—especially for more severe liver stiffness thresholds—suggests that a high number of cases may go undetected under current referral standards.
The researchers recommend that current referral pathways using FIB‑4 may need significant refinement or augmentation (e.g., with additional biomarkers or imaging tools like elastography) to better detect pre-cirrhotic liver disease in these populations.
Takeaway
FIB-4-based referral systems, while practical, may miss a sizable proportion of individuals with early to moderate liver stiffness in the general population. This underscores a need for improved screening strategies, potentially incorporating more sensitive diagnostics.
There are alternative pathways–
1. Non-Invasive Serum Biomarkers
- NAFLD Fibrosis Score (NFS) – uses BMI, age, diabetes status, ALT, AST, albumin, and platelet count. Slightly better than FIB-4 in some studies but still imperfect in general screening.
- Enhanced Liver Fibrosis (ELF) Test – measures direct fibrosis markers (hyaluronic acid, PIIINP, TIMP-1). Better sensitivity, but higher cost and less available.
- FibroTest / FibroSure – commercial blood panel combining various markers; widely used in Europe.
👉 These improve accuracy but still lack the full precision of imaging-based tools.
2. Imaging-Based Elastography
- Vibration-Controlled Transient Elastography (FibroScan®)
- Quick, point-of-care device.
- Measures liver stiffness (fibrosis) and CAP (fat content).
- More accurate than FIB-4, especially for ruling in disease.
- Widely used in hepatology clinics.
- Magnetic Resonance Elastography (MRE)
- Gold standard non-invasive stiffness measurement.
- Higher accuracy than FibroScan for detecting ≥F2 fibrosis.
- More expensive and less widely available but increasingly used.
- Shear Wave Elastography (Ultrasound-based)
- Built into many modern ultrasound machines.
- More practical in some clinical settings.
👉 Imaging adds cost, but it catches many cases that FIB-4 misses.

From NexGen, the iLivTouch® Transient Elastography (VCTE) device.
3. Two-Step Pathways
Many guidelines now recommend combining FIB-4 with an imaging test for a more balanced pathway:
- Step 1: FIB-4 as an initial screen.
- Step 2: If indeterminate or high, follow up with FibroScan or MRE.
This reduces unnecessary referrals but catches more disease than FIB-4 alone.