Summary: Acute Liver Failure: 5 Things to Know
By Eugenia Tsai, MD (May 8, 2026), and here’s the URL of the article on Medscape:
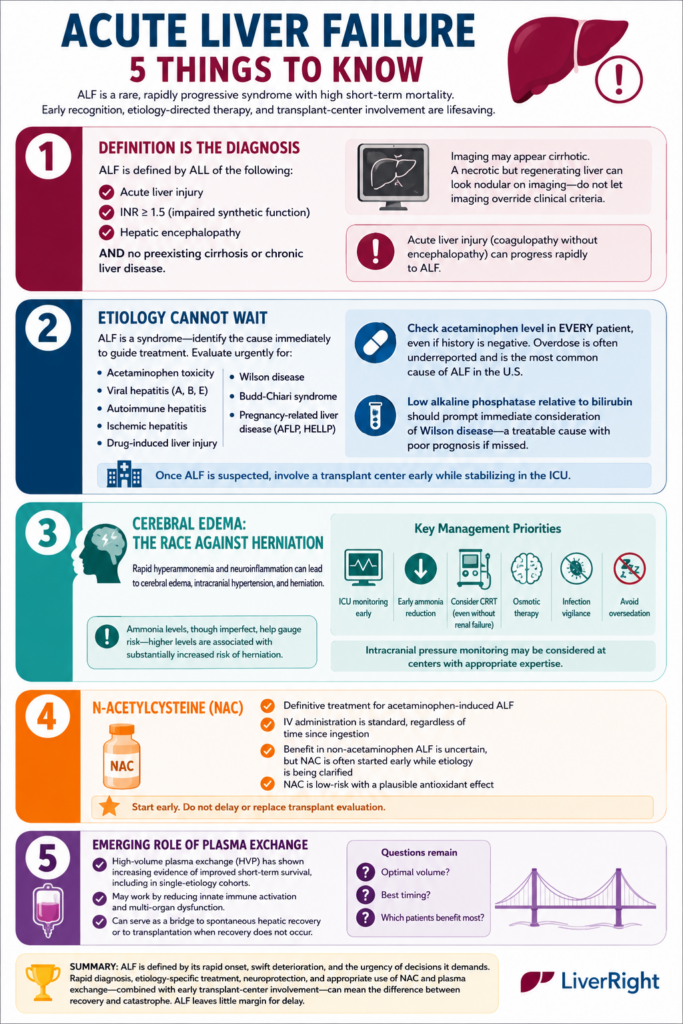
This article reviews the key clinical principles in diagnosing and managing acute liver failure (ALF) — a rare but rapidly fatal condition requiring urgent recognition, ICU-level care, and early transplant-center involvement.
1. ALF Is Defined Clinically
ALF is diagnosed by:
- Acute liver injury
- INR ≥ 1.5 (impaired synthetic function)
- Hepatic encephalopathy
- No preexisting cirrhosis or chronic liver disease
A major pitfall is that imaging may falsely resemble cirrhosis because a necrotic/regenerating liver can appear nodular. Clinical criteria should take precedence over imaging findings.
2. Determining the Cause Cannot Be Delayed
ALF is a syndrome with many causes, and treatment depends on identifying the etiology immediately. Key causes include:
- Acetaminophen toxicity
- Viral hepatitis (A, B, E)
- Autoimmune hepatitis
- Drug-induced liver injury
- Ischemic hepatitis
- Wilson disease
- Budd-Chiari syndrome
- Pregnancy-related liver disease
Two urgent diagnostic priorities:
- Check acetaminophen levels in every patient, regardless of history.
- Consider Wilson disease when alkaline phosphatase is disproportionately low relative to bilirubin.
Early transfer or consultation with a liver transplant center is emphasized.
3. Cerebral Edema Is the Major Immediate Threat
Neurologic injury distinguishes ALF from chronic liver disease. Rapid hyperammonemia and inflammation can lead to:
- Cerebral edema
- Intracranial hypertension
- Herniation
Management priorities include:
- ICU monitoring
- Early ammonia reduction
- Continuous renal replacement therapy (even without kidney failure)
- Osmotic therapy
- Avoiding oversedation
- Infection surveillance
4. N-acetylcysteine (NAC) Should Be Started Early
- NAC is the standard treatment for acetaminophen-induced ALF
- It is also frequently used in non-acetaminophen ALF, despite mixed evidence for mortality benefit
The rationale is that NAC is low-risk and may provide antioxidant and supportive benefits while the cause is being clarified. It should never delay transplant evaluation.
5. High-Volume Plasma Exchange Is Emerging as a Bridge Therapy
Recent evidence suggests high-volume plasma exchange (HVP) may improve short-term survival by:
- Reducing inflammatory mediators
- Limiting multi-organ dysfunction
HVP may serve as a bridge to:
- Spontaneous recovery
- Liver transplantation
However, questions remain about optimal timing and patient selection.
Overall Takeaway
ALF is a medical emergency with a narrow therapeutic window. Outcomes depend on:
- Rapid diagnosis
- Immediate etiology-directed treatment
- Aggressive neuroprotective management
- Early transplant-center involvement
Delays in recognition or escalation can quickly become fatal.