Here’s a clip from the article in Nature of 01/10/2025 entitled: Metabolic and alcohol-associated liver disease (MetALD): a representation of duality. The key takeaway is “MetALD is a recently coined term that refers to a systemic entity to describe patients with metabolic dysfunction-associated steatotic liver disease (MASLD) and simultaneous moderate alcohol consumption. The deleterious association of alcohol and metabolic risk factors synergistically increases the development of steatohepatitis, fibrosis, and hepatocellular carcinoma (HCC).”
Introduction: new consensus and name
Authors: Hector Leal-Lassalle, Olga Estévez-Vázquez, Francisco Javier Cubero & Yulia A. Nevzorova
“Lately, a worldwide initiative led by major pan-national liver organizations has been undertaken to rename non-alcoholic fatty liver disease (NAFLD) and non-alcoholic steatohepatitis (NASH)1,2. The new names for MASLD and MASH, respectively, stand for metabolic dysfunction-associated steatotic liver disease and metabolic dysfunction-associated steatohepatitis.
The changes are being implemented for highly legitimate reasons. Medical terminology that is felt to be “stigmatizing” should be clear steered of, regardless of its original accuracy and lack of negativity. Replacing “fatty” with “steatotic” employs a shift towards medical terminology, which is likely to increase recognition and understanding among a wider audience. Additionally, the updated terminology demonstrates a better understanding of the underlying pathophysiology of the disease as metabolic dysfunction is central to the disease pathogenesis.
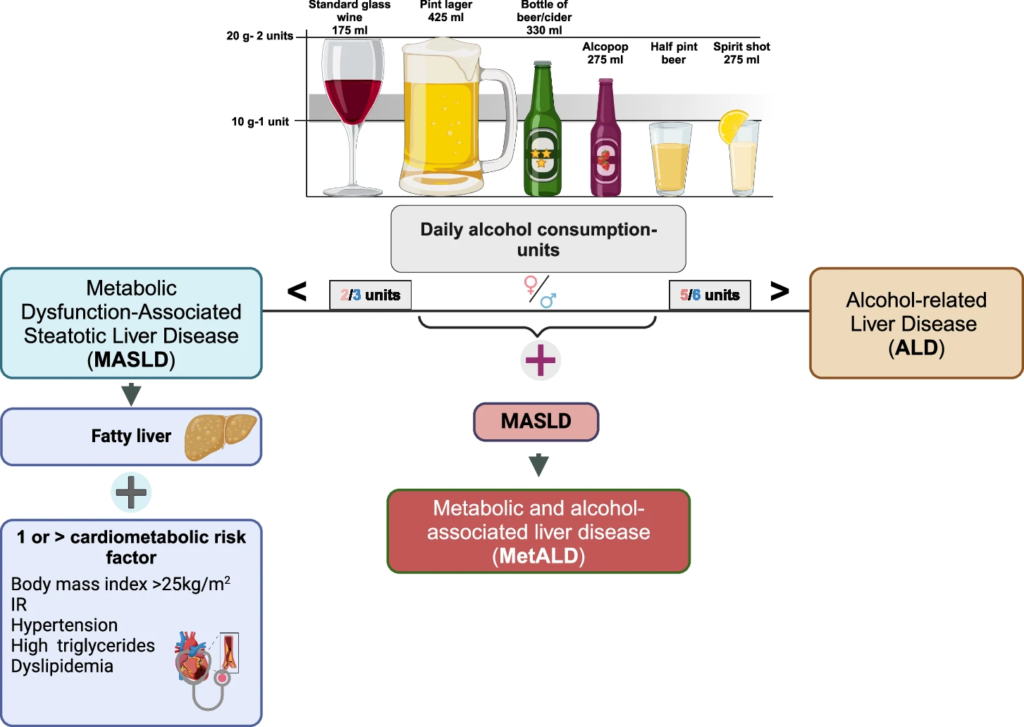
According to Delphi consensus, MASLD is diagnosed when hepatic steatosis is present along with at least one of five cardiometabolic risk factors (MRF)3. Importantly, the Delphi panel has defined and outlined a group that has not been studied before – metabolic dysfunction and alcohol associated/related liver disease (MetALD) to represent patients with MASLD and mild alcohol consumption. The patients with MetALD consume on a weekly basis 140–350 g of alcohol for females and 210–420 g for males respectively. Correspondingly, average daily alcohol consumption varies between 20–50 g for females and 30–60 g for males2,4. While measuring the amount of alcohol consumed in grams per day or week may be more accurate, it can be challenging and time-consuming to obtain this information. Widely, patients struggle to remember the types and quantities of drinks they have consumed (Fig. 1). As a result, it might be beneficial to define MetALD based on the quantity of drinks consumed. Nevertheless, there has been a significant inconsistency in defining what constitutes a “drink” in terms of alcohol grams5. Dietary guidelines for Americans6,7 and Latin American Association for the Study of the Liver (ALEH)8 define a standard drink of “pure” alcohol as 14 g. According to the British Association for the Study of the Liver/British Society of Gastroenterology (BASL/BSG)9, single standard drink of “pure” alcohol equates to 8 g. While EASL10 and WHO11 standardized it to 10 g to make comparisons among studies easier.”